
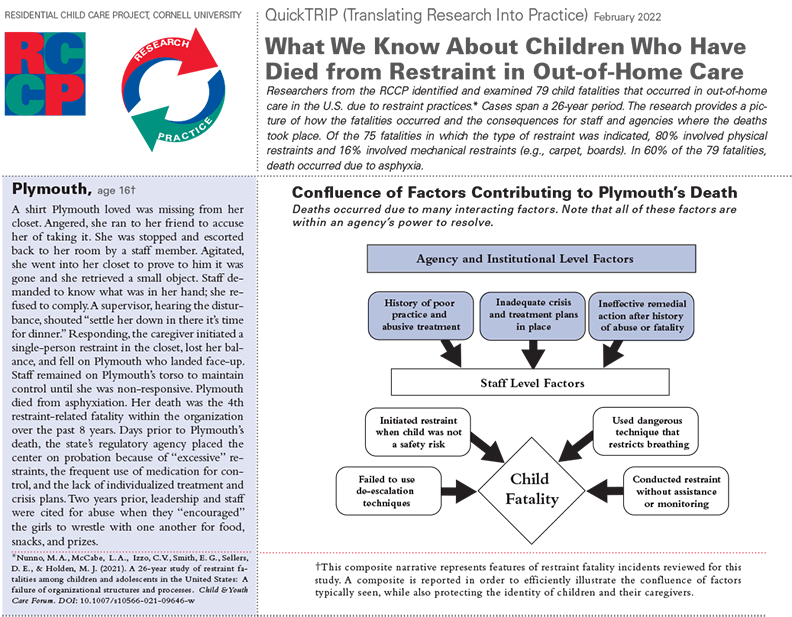
Above is page 1 of the What do We Know about Children Who Have Died from Restraint in Out-of-Home Care, QuickTRIP, February 2022. February 2022 Download the entire QuickTRIP in .pdf format.
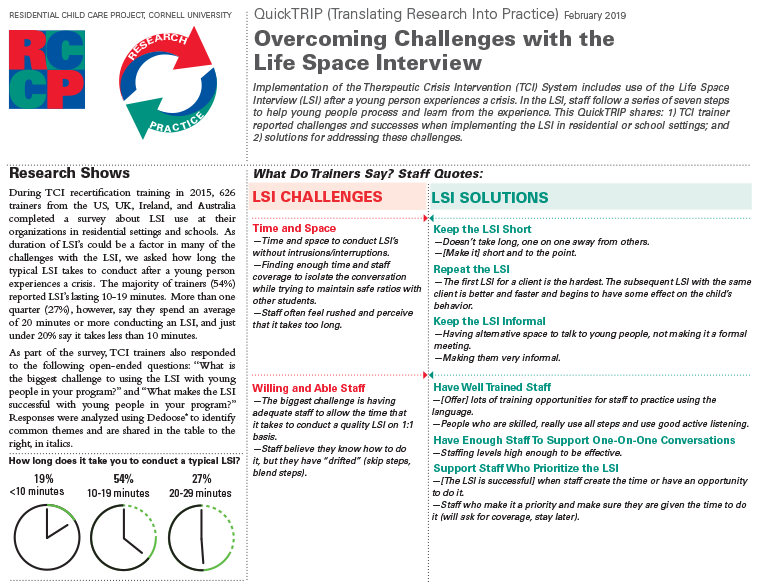
Above is page 1 of the Overcoming Challenges with the LSI QuickTRIP, February 2019. Download the entire QuickTRIP in .pdf format.
McCabe, L. A., Ruberti, M. R., & Endres, T. (2022). Sustaining program implementation: A co-constructed technical assistance process to support continuous high-quality implementation of the Therapeutic Crisis Intervention program. Evaluation and Program Planning, 91, 102049.
Strategies for sustaining a program beyond initial implementation remain one of the most poorly understood aspects of high-quality program implementation. This paper describes the Quality Improvement and Fidelity Assessment Process (QIFAP), a program purveyor-agency partnership that uses a unique, multi-step method for supporting sustained implementation of the Therapeutic Crisis Intervention (TCI) system to manage crises in child serving organizations. It outlines the steps of the process and highlights how specific activities are linked to current knowledge and principles from implementation science. The QIFAP occurs over a period of about three months, during which time program developers and agency representatives conduct staff surveys, a two-day site visit, and fidelity assessments in order to gather information, discuss findings, and plan steps for improving the TCI system in the organization. The process is guided by principles that emphasize the importance of organization leadership, building relationships, co-learning, using an individualized approach, data informed decision making, acknowledging risk, and congruence. We describe ways in which the strategies and approaches within the QIFAP are rooted in implementation science literature. Thus, the model represents an illustration of how research-based knowledge can work in practice to support long-term, high-quality program implementation.
Izzo, C. V., Smith, E. G., Sellers, D. E., Holden, M. J., & Nunno, M. A. (2022). Promoting a relational approach to residential child care through an organizational program model: Impacts of CARE implementation on staff outcomes. Children and Youth Services Review, 132, 106330. https://doi.org/10.1016/j.childyouth.2021.106330
We evaluated the impact of Children and Residential Experiences (CARE), an organization-wide program model implemented in 13 residential child care agencies in one Southeastern state. CARE implementation lasted three years and involved the application of six evidence-informed principles throughout the organization in order to create more therapeutic environments and improve the quality of care for children. A wait-list design was used with one cohort of agencies starting CARE immediately and a second cohort waiting 12 months before starting, allowing them to serve as a comparison group. Agency staff completed annual surveys assessing curricular knowledge, their beliefs about and their use of practices that reflect a relational approach to care. Using linear mixed models that accounted for clustering within agencies and several important covariates, results showed significant increases in all staff outcomes. CARE effects on knowledge and beliefs emerged in Year 1 and CARE effects on practice emerged in Year 3. Exploratory analyses showed that the CARE effects were evident across all staff demographic and agency subgroups, with evidence of more pronounced effects for some subgroups. Results contribute to an emerging pattern of evidence that CARE implementation improves the capacity of agencies to provide effective therapeutic care for children.
Nunno, M. A., McCabe, L. A., Izzo, C. V., Smith, E. G., Sellers, D. E., & Holden, M. J. (2021). A 26-Year Study of Restraint Fatalities Among Children and Adolescents in the United States: A Failure of Organizational Structures and Processes. Child & Youth Care Forum. https://doi.org/10.1007/s10566-021-09646-w
Background
Physical and mechanical restraints used in treatment, care, education, and corrections programs for children are high-risk interventions primarily due to their adverse physical, emotional, and fatal consequences.
Objective
This study explores the conditions and circumstances of restraint-related fatalities in the United States by asking (1) Who are the children that died due to physical restraint? and (2) How did they die?
Method
The study employs internet search systems to discover and compile information about restraint-related fatalities of children and youth up to 18 years of age from reputable journalism sources, advocacy groups, activists, and governmental and non-governmental agencies. The child cohort from a published study of restraint fatalities in the United States from 1993 to 2003 is combined with restraint fatalities from 2004 to 2018. This study’s scope has expanded to include restraint deaths in community schools, as well as undiscovered restraint deaths from 1993 to 2003 not in the 2006 study.
Results
Seventy-nine restraint-related fatalities occurred over the 26-year period from across a spectrum of children’s out-of-home child welfare, corrections, mental health and disability services. The research provides a data snapshot and examples of how fatalities unfold and their consequences for staff and agencies. Practice recommendations are offered to increase safety and transparency.
Conclusions
The study postulates that restraint fatalities result from a confluence of medical, psychological, and organizational causes; such as cultures prioritizing control, ignoring risk, using dangerous techniques, as well as agencies that lack structures, processes, procedures, and resources to promote learning and to ensure physical and psychological safety.
Sellers, D. E., Smith, E. G., Izzo, C. V., McCabe, L. A., & Nunno, M. A. (2020). Child feelings of safety in residential care: The supporting role of adult-child relationships. Residential Treatment for Children & Youth, 37(2), 136–155. https://doi.org/10.1080/0886571X.2020.1712576
For children in residential care, safety and supportive relationships, particularly with direct care staff, are critical to recovery, growth, and development. The association between children?s self-report of feeling safe and of the quality of relationships with staff was examined in 715 children ages 8?21 receiving care in 24 North American agencies. In total, 64% of children report usually or always feeling safe, 16% report never or rarely feeling safe, and 20% feel safe sometimes. The percentage of children reporting never or rarely feeling safe varied from 0% to 57% across agencies. Staff perceptions of child safety were greater than those of the children. After controlling for child and agency covariates, the quality of the relationship with staff as perceived by the children was highly associated with the extent to which the child reported feeling safe. No child demographic, service history, or agency characteristics were associated with children perceptions of safety in the linear mixed model that included quality of relationship with staff. Staff practices, fostered and sustained by organizational support, that improve the quality of their relationships with children may increase children's feelings of safety and thus their capacity for benefiting from therapeutic residential care.
Izzo, C. V., Smith, E. G., Sellers, D. E., Holden, M. J., & Nunno, M. A. (2020). Improving relationship quality in group care settings: The impact of implementing the CARE model. Children and Youth Services Review, 109. https://doi.org/10.1016/j.childyouth.2019.104623
The current study examined the effects of implementing a new program model on the quality of relationships between direct care providers and residents in group care agencies. Children and Residential Experiences (CARE), an organization-wide program model that involves a range of structural change and staff-development activities, was implemented in 13 group care agencies in one Southeastern state. CARE implementation lasted three years and involved the application of six evidence-informed principles throughout the organization in order to create more therapeutic environments and improve the quality of care for children. We used a stepped-wedge design in which one cohort of agencies began CARE immediately and a second cohort waited 12 months before beginning, allowing them to serve as a comparison group during the waiting period. Children in each agency were surveyed annually about the perceived quality of their relationships with staff using a new instrument developed for this study. Results of a linear mixed model indicated that after accounting for clustering at the agency and cottage levels and controlling for several important covariates, child perceptions of relationship quality increased significantly in the three years after CARE implementation began. The strength of the CARE effect was stronger for residents with several previous placements, but did not differ by age, gender, race, length of stay, DSS referral, or problem behavior. Results provide evidence that supports the effectiveness of CARE as an intervention to help group care agencies improve the quality of children’s daily interactions with caregiving staff, a critical aspect of their experience while living in care. The process requires a long-term commitment and an organization-wide focus on serving the best interests of children.
LeBel, J., Holden, M. J., Fauntleroy, D. A., Galyean, L., Martin, W. R., & Casciano-McCann, C. (2020). Residential transformation: Successful strategies and examples. In B. Caldwell, R. E. Lieberman, J. LeBel, & G. M. Blau (Eds.), Transforming residential interventions: Practical strategies and future directions. Routledge. https://www.taylorfrancis.com/books/9781351187473
This chapter illustrates through program-specific examples the exciting ways that residential transformation is occurring. Residential leaders are being compelled to reform, elevate their practice, and deliver effective interventions. Funders, regulators, and oversight agencies are not just interested in purchasing beds; rather on buying sustained positive outcomes for the youth and families served. As a result, innovative providers are delivering transformative change through visionary goal-oriented leadership; focused workforce support and development; active youth and family engagement; and a strong commitment to service that is trauma-informed, culturally and linguistic competent, data and quality-driven, and fiscally flexible. An in-depth discussion of three different organizations’ change processes, including specific actions taken, challenges encountered, and lessons learned is provided. Each leader recognizes their transformation journey is ongoing, fueled by urgency, and grounded in family and community connection. Moreover, each leader offers their professional contact information for readers seeking more information.
Holden, M. J., & Sellers, D. (2019). An evidence-based program model for facilitating therapeutic responses to pain-based behavior in residential care. International Journal of Child, Youth and Family Studies, 10(2–3), 63–80. https://doi.org/10.18357/ijcyfs102-3201918853
Children and young people in residential care have often lived lives saturated with loss, neglect, rejection, and traumatic experiences. Children express the pain of trauma in various ways, namely pain-based behaviors manifesting in ways that often leave their care givers confused, frustrated, frightened, angry or exhausted. For residential caregivers to respond to children and young people in a consistent and therapeutic manner, residential environments must provide an ethos of respect, caring, and trust, creating a safe place for children and staff to live and learn together. This paper describes the Children and Residential Experiences (CARE) model, its implementation, and evidence for its effectiveness. CARE is a trauma-informed, principle-based, multi-component program designed to enhance the social dynamics in group care settings and help agencies create a living environment that provides developmentally enriching experiences for children in their care. By incorporating the CARE principles throughout all levels of the organization and into daily practice, the CARE program model has been shown to improve the capacity of staff to establish positive developmental relationships with the children in their care, offer developmentally enriching experiences and a “sense of normality”, and create cohesion and congruence throughout the organization. Through consistent and predictable compassionate and responsive interactions with adults, as well as opportunities to overcome challenges and to experience successful learning opportunities, children can grow, develop and thrive.
Holden, M. J. (2019). A Collection of notions about The Other 23 Hours. Residential Treatment for Children & Youth, 36(1), 21–26. https://doi.org/10.1080/0886571X.2018.1515604
Being invited to write this commentary is a career high. To prepare, I took an old and tattered autographed copy of The Other 23 Hours down from my bookshelf. It had been many years since I had read this book. When I first read it, I was a young clinician at a residential center. Thinking back on my "beginnings" I recalled how this book had changed my perspective of my job. My "aha" moment was that I was not a therapist hired to work individually with emotional troubled children but, instead, I was part of a team. I could play a valuable role in helping staff understand children's behaviors. I could design activities and responses to help children learn new adaptive behaviors! At that time and in that moment, The Other 23 Hours changed my ideas about how residential care could impact children's lives. After reflecting on my first reading, I opened the book and, much to my surprise, this reading became an even more personal journey through my career.
Nunno, M. A., Smith, E. G., Martin, W. R., & Butcher, S. (2017). Benefits of embedding research into practice: An agency-university collaboration. Child Welfare, 94(3), 113–133.
The present study describes the efforts of an agency-university partnership to support the use of research evidence to improve the interactional quality among staff and youth in therapeutic residential care. Using 12 years of administrative data, time series analyses are used to measure changes and guide remedial actions associated with the implementation of a program model across three service populations within an agency. The study illustrates ways in which agencies can collaborate with researchers to enhance use of their own data and incorporate knowledge from research into their practice to improve the experience for children in residential treatment settings.
Izzo, C. V., Smith, E. G., Holden, M. J., Norton, C. I., Nunno, M. A., & Sellers, D. E. (2016). Intervening at the setting level to prevent behavioral incidents in residential child care: Efficacy of the CARE program model. Prevention Science, 17(5), 554–564. https://doi.org/10.1007/s11121-016-0649-0
The current study examined the impact of a setting-level intervention on the prevention of aggressive or dangerous behavioral incidents involving youth living in group care environments. Eleven group care agencies implemented Children and Residential Experiences (CARE), a principle-based program that helps agencies use a set of evidence-informed principles to guide programming and enrich the relational dynamics throughout the agency. All agencies served mostly youth referred from child welfare. The 3-year implementation of CARE involved intensive agency-wide training and on-site consultation to agency leaders and managers around supporting and facilitating day-to-day application of the principles in both childcare and staff management arenas. Agencies provided data over 48 months on the monthly frequency of behavioral incidents most related to program objectives. Using multiple baseline interrupted time series analysis to assess program effects, we tested whether trends during the program implementation period declined significantly compared to the 12 months before implementation. Results showed significant program effects on incidents involving youth aggression toward adult staff, property destruction, and running away. Effects on aggression toward peers and self-harm were also found but were less consistent. Staff ratings of positive organizational social context (OSC) predicted fewer incidents, but there was no clear relationship between OSC and observed program effects. Findings support the potential efficacy of the CARE model and illustrate that intervening “upstream” at the setting level may help to prevent coercive caregiving patterns and increase opportunities for healthy social interactions.
Whittaker, J. K., Holmes, L., Valle, J. F. del, Ainsworth, F., Andreassen, T., Anglin, J., Bellonci, C., Berridge, D., Bravo, A., Canali, C., Courtney, M., Currey, L., Daly, D., Gilligan, R., Grietens, H., Harder, A., Holden, M., James, S., Kendrick, A., … Zeira, A. (2016). Therapeutic Residential Care for Children and Youth: A Consensus Statement of the International Work Group on Therapeutic Residential Care*. Residential Treatment for Children & Youth, 33(2), 89–106. https://doi.org/10.1080/0886571X.2016.1215755
In many developed countries around the world, “group care’’ interventions for children and adolescents have come under increasing scrutiny from central government, private philanthropic, and child advocacy agencies desirous of:
- achieving better outcomes for vulnerable children and youth;
- doing so in closer collaboration with their families and in closer proximity to their home communities and cultures in ways that reduce the potential for abuse while maximizing the use of informal helping resources; and,
- with the hope of reducing the high costs often associated with group residential provision.
In some jurisdictions, efforts to reduce residential care resources in the absence of sufficient alternatives to serve high-resource needing youth has had unintended and negative consequences (Ainsworth & Hansen, 2005). Underpinning these many reform efforts has been a widely shared desire to design interventions that are effective and consistent with what is known about avoiding iatrogenic effects such as “deviancy training’’ and providing multiple opportunities for children to progress to the full limit of their developmental potential wherever they are served. Robbie Gilligan from Trinity College, Dublin has succinctly illuminated the challenges confronting those who seek to identify a place and purpose for high quality therapeutic residential care services in an overall child and family services system (Gilligan, 2014).
The International Work Group for Therapeutic Residential Care convened an International Summit on ‘Pathways to Evidence-Based Practice’ at Loughborough University (GBR), Centre for Child and Family Research on 27-29 April, 2016 with generous support from the Sir Halley Stewart Trust and in partnership with The European Scientific Association on Residential and Family Care for Children and Adolescents (NLD) (EUSARF), the International Association for Outcome-Based Evaluation and Research on Family and Children’s Services (ITA) (IAOBER) and the Association of Children’s Residential Centers (USA) and with the additional support of Action for Children (GBR) and the National Implementation Service (NIS) (GBR).
Holden, M., Anglin, J. P., Nunno, M. A., & Izzo, C. V. (2014). Engaging the total therapeutic residential care program in a process of quality improvement: Learning from the CARE model. In J. K. Whittaker, J. F. Del Valle, & L. Holmes (Eds.), Therapeutic residential care for children and youth: Identifying promising pathways to evidence-based international practice. Jessica Kingsley.
Recent questioning of the appropriateness of residential care has led to the need for a clearer assessment of the scope, purpose, fit, and cost of group care and its relevance and utility to a community’s child welfare system (Ainsworth and Hansen 2005; Delap 2011; Noonan and Menashi 2010). As pointed out by the editors of this text, there is a need to define and build a foundation for quality child welfare services that use Therapeutic Residential Care (TRC) judiciously through a comprehensive assessment process and “for only high-need children and youth with multiple challenges inactive collaboration with the full suite of empirically based family- and community-centered programs” (Whittaker, del Valle, and Holmes, Chapter 1, this volume, p.26).
We have defined three core concepts to guide quality therapeutic residential services provided by any organization or community child welfare system. These concepts include the best interests of children, organizational congruence, and an explicit program model, and their implementation depends on varying levels of professional sophistication, discipline dependent knowledge, and existing “theories in use”.
Izzo, C. V., Aumand, B. N., Cash, B. M., McCabe, L. A., Holden, M. J., & Bhattacharjee, M. (2014). Exploration of the youth-adult relationship in residential care: Small glimpses from a large sample of youth. International Journal of Child and Family Welfare, 15(1/2), 10–23.
This study examined the perceptions of youth living in residential care about their relationships with the youth care workers who care for them. The data come from an open-ended survey question asking youth to describe the qualities they like about their favorite youth care worker. A total of 738 youth from across 16 agencies participated, and a wide range of topics were described. Using the constant comparative method, we developed a scheme for categorizing care worker qualities and coded all responses to identify the primary themes reported by youth. Eighteen categories emerged including qualities mostly related to interactional style such as engagement, genuineness, flexibility, understanding, respect, and structure. The categories endorsed by youth differed based on their gender, age, and tenure at the agency. Findings from this work can support residential care agencies’ efforts to maximize their fit with the needs, preferences, and best interests of the youth they serve.
Nunno, M. A., Sellers, D. E., & Holden, M. J. (2014). Implications of translational research for the field of residential child care. Scottish Journal of Residential Child Care, 13(3).
This article will address a brief history of the nature and definition of translational research and introduce several relevant debates within the field of translational research, specifically the relationship between practice-based knowledge and research in therapeutic residential child care. We offer a model of translational research developed by Hamilton (2014), particularly for work related to youth development that has the potential to bring the child care practitioner to the centre of the process to improve the outcomes of high-needs children. Finally, we provide some lessons learned from the implementation and evaluation of two major programmes designed to improve the quality of therapeutic residential care.
Masters, K. J., Nunno, M., & Mooney, A. J. (2013). Should psychiatrists assist in the restraint of children and adolescents in psychiatric facilities? Psychiatric Services, 64(2), 173–176. https://doi.org/10.1176/appi.ps.001652012
Psychiatrists in psychiatric hospitals or residential facilities can find themselves involved in patient crises that precipitate a restraint or seclusion. The decision to become directly involved must be made quickly, with little time for administrative or legal consultation. The psychiatrist’s decision to participate in physically restraining or secluding a patient, particularly a child or adolescent, may have long-lasting consequences. This Open Forum is offered to promote a discussion on this topic. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Holden, M. J., Holden, J. C., & Sandy, P. (2012). Developing Preventative Responses to Disruptive and High-Risk Behaviours. In J. Visser, H. Daniels, & T. Cole (Eds.), Transforming Troubled Lives: Strategies and Interventions for Children with Social, Emotional and Behavioural Difficulties (Vol. 2, pp. 309–322). Emerald Group Publishing Limited. https://doi.org/10.1108/S1479-3636(2012)0000002022
Disruptive and potentially unsafe classroom behaviours such as threatening, bullying, verbal and/or physical assaulting present challenges not only for teachers, aides and other students in the classroom, but potentially for all others in the building as well as the families of those students/pupils involved. These behaviours can greatly influence a student's ability to achieve academic success as well as place undue stress and risk on others in the milieu.
Discovering the cause for the behaviours and then developing a plan to help these young people succeed emotionally will greatly increase the probability for improved academic achievement. This chapter will examine the core principles of the Therapeutic Crisis Intervention for Schools (TCIS) programme and present a range of evidence-based responses designed to help build upon and further develop staff skills in preventing disruptive behaviours, de-escalating potential disruptive behaviours, and teach students how to develop less disruptive and more appropriate responses to their lack of or inability to self-regulate.
This chapter will contend that the foundation for all interventions and responses presupposes an accurate assessment of risk for the youth(s), the adults, and the environment. That any risk assessment must consider the internal (effects of trauma, ability to self-regulate, cultural issues) and external (organizational culture/climate, level of restrictiveness, caring community, quality of instruction) setting conditions for the youth.
The TCIS programme is embedded in the five domains for effective crisis management; leadership and building support, social work and clinical services participation (social workers, psychologists, therapists, nurses), building administration and post crisis response, training and competency standards, and data-driven incident monitoring and feedback.
LeBel, J., Nunno, M. A., Mohr, W. K., & O’Halloran, R. (2012). Restraint and seclusion use in US School settings: Recommendations from allied treatment disciplines. American Journal of Orthopsychiatry, 82(1), 75–86. https://doi.org/10.1111/j.1939-0025.2011.01134.x
Restraint and seclusion (R&S) are high risk, emergency procedures that are used in response to perceived violent, dangerous situations. They have been employed for years in a variety of settings that serve children, such as psychiatric hospitals and residential treatment facilities, but are now being recognized as used in the public schools. The field of education has begun to examine these practices in response to national scrutiny and a Congressional investigation. The fields of mental health and child welfare were similarly scrutinized 10 years ago following national media attention and have advanced R&S practice through the adoption of a prevention framework and core strategies to prevent and reduce use. A review of the evolution of the national R&S movement, the adverse effects of these procedures, and a comprehensive approach to prevent their use with specific core strategies such as leadership, workforce development, and youth and family involvement in order to facilitate organizational culture and practice change are discussed. Proposed guidelines for R&S use in schools and systemic recommendations to promote R&S practice alignment between the child‐serving service sectors are also offered. (PsycINFO Database Record (c) 2017 APA, all rights reserved)
Mohr, W. K., & Nunno, M. A. (2011). Black boxing restraints: The need for full disclosure and consent. Journal of Child and Family Studies, 20(1), 38–47. https://doi.org/10.1007/s10826-010-9375-6
In this article we discuss the necessity of fully informing patients and their families of what constitutes physical interventions and their attendant risks under the established principles and obligations of informed consent. After a brief review of the elements of informed consent and the nature of the duty to advise patients and their families of treatment risks, we argue that physical interventions are an unvalidated treatment for aggressive and violent behavior and should be used only as a safety intervention. We focus our discussion on the informed consent issues for school aged children, adolescents, and emancipated minors and contend that if restraints are used they must pose less risk than the behavior they are trying to alleviate. We also opine that if restraints are misused by mental health or child welfare treatment settings, then their misuse may be considered a subject of a patient maltreatment, abuse, criminal or civil action. A central thesis of the article is that informed consent must be seen as an integral and dynamic process of treatment. We recommend strategies that gain parental permission and child assent, that view informed consent as a dynamic and individualized process that aids and supports the therapeutic relationship, and that stress the importance of simplicity and clarity. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Nunno, M. (2011). Climate control: Whether an organisation is healthy or toxic is dictated by its leadership style. Learning Disability Practice, 14(6), 11. https://link.gale.com/apps/doc/A262602834/HRCA?u=cornell&sid=bookmark-HRCA&xid=19878111
The nature of nurses’ work puts them in close proximity to patients and therefore makes them vulnerable to aggression and violence. Although efforts have been made to reduce the potential for physical abuse in nursing homes and other treatment facilities, the frequency and seriousness
of injuries to staff indicates that it is an on-going problem.
Nurses are responsible for patient safety and to ensure this, nurses often have to use interventions such as physical restraint that carry inherent risks for the patient and nurse. The question is, does the intervention or event have more risk than the behaviour we are trying to control or contain.
Although this seems like a simple question, the culture and the climate of the organisation often determines the answer.
Holden, M., Izzo, C., Nunno, M., Smith, E., Endres, T., Holden, J., & Kuhn, F. (2010). Children and Residential Experiences: A comprehensive strategy for implementing a research-informed program model for residential care. Child Welfare, 89(2), 131–149.
This paper describes an effort to bridge research and practice in residential care through implementing a program model tided Children and Residential Experiences (CARE). The strategy involves consulting at all levels of the organization to guide personnel to incorporate CARE evidence-based principles into daily practice, and fostering an organizational culture and climate that sustains the integration of CARE principles. CARE aims to promote residential care programs that serve the best interests of children.
Nunno, M. (2009). Invited commentary on “CAPTA and the residential placement: A survey of state policy and practice.” Child & Youth Care Forum, 38(2), 69–73. https://doi.org/10.1007/s10566-009-9068-8
Comments on an article by Mary Ann Overcamp-Martini and Jennifer S. Nutton (see record [rid]2009-04185-001[/rid]). The article points out that state and national protection and advocacy centers for persons with mental illness and developmental disabilities have been in the forefront of needed system and legislative initiatives to protect children in care and that the child welfare, social work, and juvenile justice professions have been late in coming to these legislative initiatives. As is stated in the article, there should be additional specialized prevention and intervention systems necessary to hold providers to higher standards than those necessary for parents. Duty demands that professional providers recognize basic risks to the child population that they serve, and that these professionals foresee and prevent unnecessary risks that may cause harm or a risk of harm. Personal safety is a basic need and fundamental right for compromised children. Anything less can be considered abusive or neglectful practice by the facility. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Holden, M. (2009). Children and residential experiences (CARE): Creating conditions for change. Child Welfare League of America.
To obtain a copy of this book, click the link below.
Holden, M. J., & Curry, D. (2008). Learning from the research. In M. A. Nunno, D. M. Day, & L. B. Bullard (Eds.), For our own safety: Examining the safety of high-risk interventions for children and young people. Child Welfare League of America.
This chapter outlines how the RCCP team took lessons learned from an independent study of TCI Trainer’s ability to consistently rate TCI physical restraint skills and applied these findings and other relevant research to the redevelopment of the TCI training curriculum for the 5thedition of TCI.
Nunno, M. A., Day, D. M., & Bullard, L. B. (Eds.). (2008). For our own safety: Examining the safety of high-risk interventions for children and young people. Child Welfare League of America.
“For Our Own Safety” is devoted entirely to the subject of, and risks associated with, restraint and seclusion of children. This book is a collection of the diverse viewpoints presented at the international symposium, “Examining the Safety of High-Risk Interventions for Children and Young People” (Ithaca, New York, June 1-4, 2005). It presents frank examination of the legal, ethical, and historical uses of physical restraints and seclusion. Also addressed in this collection are issues of safety, the psychological and emotional impacts of restraint, guidelines for development and use, as well as clinical and organizational strategies likely to reduce use. Intended for use by professionals who want to address the impact of aggression and violence in residential care, this volume contributes to the discussion of the appropriate use of high-risk interventions and the ways to improve the general quality of child residential treatment services though safe and harm-free environments. Following a foreword by Jaap E. Doek, the book contains six parts. Part I, Young People and Physical Restraints, presents: (1) Young People’s Experiences of Physical Restraint in Residential Care: Subtlety and Complexity in Policy and Practice (Laura Steckley and Andrew Kendrick). Part II, Theoretical and Historical Issues, continues with: (2) Literature on the Therapeutic Effectiveness of Physical Restraints with Children and Youth (David M. Day); and (3) Modernizing Seclusion and Restraint (Kim J. Masters). Part III, Ensuring Safety and Managing Risk, contains: (4) Physical Restraints: Are They Ever Safe and How Safe Is Safe Enough? (Wanda K. Mohr); (5) Risk and Prone Restraint: Reviewing the Evidence (David Allen); and (6) Learning from the Research (Martha Holden and Dale Curry). Part IV, Reducing Restraints through Organizational Change, contains: (7) Adopting a Public Health Model to Reduce Violence and Restraints in Children’s Residential Care Facilities (Brodie Paterson, David Leadbetter, Gail Miller, and John Crichton); (8) Leadership’s and Program’s Role in Organizational and Cultural Change to Reduce Seclusions and Restraints (David Colton); (9) A Case Study Organizational Intervention to Reduce Physical Interventions: Creating Effective, Harm-Free Environments (Ronald W. Thompson, Jonathan C. Huefner, Dennis G. Vollmer, Jerry L. Davis, and Daniel L. Daly); (10) Beyond a Crisis Management Program: How We Reduced Our Restraints by Half in One Year (Jeff Carter, Judy Jones, and Kim Stevens); (11) Reducing the Use of Seclusion and Restraint in a Day School Program (Joseph B. Ryan, Reece L. Peterson, George Tetreault, and Emily van der Hagen); and (12) Lessons Learned from 30 Plus Years of No Physical Intervention (George Suess). Part V, Legal Issues, contains: (13) Using Restraint: The Legal Context of High-Risk Interventions (Sheila Suess Kennedy); and (14) The Reach of Liability for Restraints: A Question of Professional Judgment (Andrea J. Mooney). Part VI, Conclusion, completes the book with: (15) Moving Forward (David M. Day, Lloyd B. Bullard, and Michael A. Nunno). An index is included.
Leidy, B. D., Haugaard, J. J., Nunno, M. A., & Kwartner, J. K. (2006). Review of restraint data in a residential treatment center for adolescent females. Child & Youth Care Forum, 35(5–6), 339–352. https://doi.org/10.1007/s10566-006-9021-z
This paper presents a review of the physical restraints that occurred at a northeastern United States residential treatment facility for adolescent females from January 1999 to May 2002. During this period, the facility housed 415 adolescents and reported 1,059 physical restraints involving 155 of them. This report assesses the characteristics of the adolescents housed at the facility, the frequency and nature of the restraints they experienced, and the relationship between the adolescents’ characteristics and the frequency with which they were restrained. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Nunno, M. A., Holden, M. J., & Tollar, A. (2006). Learning from tragedy: A survey of child and adolescent restraint fatalities. Child Abuse & Neglect, 30(12), 1333–1342. https://doi.org/10.1016/j.chiabu.2006.02.015
Objective: This descriptive study examines 45 child and adolescent fatalities related to restraints in residential (institutional) placements in the United States from 1993 to 2003.MethodThe study team used common Internet search engines as its primary case discovery strategy to determine the frequency and the nature of the fatalities, as well as the characteristics of the children and the adolescents involved. Results: Male children and adolescents were over-represented in the study sample. Thirty-eight of the fatalities occurred during or after a physical restraint, and 7 fatalities occurred during the use of mechanical restraints. Twenty-eight of the deaths occurred in a prone restraint. In 25 of the fatalities, asphyxia was the cause of death. Conclusion: In the 23 cases in this study where information is available, none of the child behaviors or conditions that prompted the restraint would meet the standard of danger to self or others: the commonly accepted criteria for the use of a restraint. The study points to deficiencies in fatality reporting, recommends reporting fatalities to established state child fatality review boards, and reinforces that restraints be governed by strict protocol and monitoring. The study also urges caution to policymakers in substituting or changing restraint procedures based on the incomplete data reported in this study.
Nunno, M. (2006). Invited commentary on “The effects of the ARC organizational intervention on caseworker turnover, climate, and culture in children’s services systems.” Child Abuse & Neglect, 30(8), 849–854. https://doi.org/10.1016/j.chiabu.2006.03.001
Comments on the article by Glisson et al (see record #200611672-003). Recent studies by the Child Welfare League of America (Child Welfare League of America, 2002) and the United States General Accounting Office (United States Government Accounting Office, 2003) address the reality of the increasing number of children needing public child welfare services with the corresponding lack of qualified staff to provide these services. The study by Glisson, Dukes, and Green (2006) reported in this issue tests a randomly assigned organizational intervention strategy, called the Availability, Responsiveness, and Continuity (ARC) program, on the organizational climate, culture, and turnover of community-based public child welfare agencies. The research is a reminder of the complex yet ambiguous tasks of child welfare work. Life as a child welfare caseworker is given to role ambiguity, overload, exhaustion, and conflict. Any quality professional service provided demands an organizational climate in congruence with and supportive of that service. Another lesson in this study is that organizational culture cannot be changed rapidly and without long-term strategies. One of the goals of research is replication (or comparison) of effects with similar or dissimilar interventions. This article acknowledges that professional child welfare practice is provided within the characteristics and climate of organizational settings. (PsycINFO Database Record (c) 2016 APA, all rights reserved).
Nunno, M. A., Holden, M. J., & Leidy, B. (2003). Evaluating and monitoring the impact of a crisis intervention system on a residential child care facility. Children and Youth Services Review, 25(4), 295–315. https://doi.org/10.1016/S0190-7409(03)00013-6
Residential child care staff require specialized knowledge and skills to prevent and manage aggressive and acting out behavior on the part of children in their care. Often a child's aggression is visible through crisis episodes that leave both the child and the care worker in turmoil. Without proper training and supervisory support, staff can react to a child's aggression with counter-aggression; or worse, staff can respond with abusive behavior toward the child. This article reports the process and impact of implementing a consistent crisis intervention methodology known as Therapeutic Crisis Intervention (TCI) within one medium sized facility in the northeastern United States. Impact was measured by monitoring critical incidents, staff knowledge, confidence and skill levels, and the consistency of staff intervention pre and post implementation. The implementation of TCI was successful in substantially reducing critical incidents, significantly reducing documented physical restraint episodes in one unit, and increasing staff knowledge, confidence and consistency in crisis intervention facility-wide. The article discusses the limitations of this evaluation and monitoring system, and suggests additional evaluation strategies that might overcome these limits.
Nunno, M. A. (1996). Monitoring and evaluating a therapeutic crisis intervention methodology in a residential child care facility [Dissertation, City University of New York]. https://www.proquest.com/dissertations-theses/monitoring-evaluating-therapeutic-crisis/docview/304294749/se-2?accountid=10267
The purpose of this project is to implement, monitor and evaluate a crisis prevention and crisis management program into a residential treatment setting. The primary goals of the crisis prevention and management program, known as the Cornell University’s Therapeutic Crisis Intervention project, are to: (1) provide the direct care worker with skills and knowledge to help children change maladaptive patterns of behavior; (2) de-escalate crises and to present strategies for dealing with upset children; (3) use crisis as an opportunity for children to learn new coping skills; (4) teach safe, appropriate physical restraint and self-protection techniques. Throughout the life of this 18 month project, interviews were conducted, questionnaires were distributed, and critical incident reports were collected. An advisory group met with the implementation and evaluation staff from Cornell University to facilitate the project. The project developed a triangulated evaluation methodology. During the first phase of this project prior to implementation staff collected critical incident reports for baseline data, and developed a computer based data collection instrument to input the present critical incidents, and to assist in monitoring, measuring and analysis. Confidence questionnaires were administered and interviews conducted assessing current practice and staff attitudes. During the second phase of this project four trainers from the facility attended a five day Training of Trainers in Therapeutic Crisis Intervention program. Upon their return, all levels of the residential child care personnel attended TCI training. In addition, supervisors attended a special session to learn specific implementation, monitoring and supervisory methods to support implementation. The third phase, project staff conducted interviews, administered confidence and knowledge based tests to monitor implementation. Critical incident monitoring continued through this phase. Technical assistance was available throughout the period. Post implementation critical incident data was collected and contrasted to the critical incidents collected during the baseline period. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Nunno, M. A. (1997). Institutional abuse: The role of leadership, authority and the environment in the social sciences literature. Early Child Development and Care, 133, 21–40. https://doi.org/10.1080/0300443971330103
Conducted a literature review to examine the variables associated with child maltreatment in 24 hr out-of-home care. Maltreatment was defined in this study as the foreseeable injury, probable injury, foreseeable harm, or probable harm to the child’s physical, social, intellectual, emotional, or developmental well-being. The residential care environment was examined with respect to the organizational culture established by the administration, the system of care, supervision patterns, and staffing patterns. The review also examined the age, gender, education, background, training, status in the facility, attitudes, job stress of each caregiver as well as child and exogenous factors. This review found that training child care workers in approved crisis intervention and crisis management strategies is essential. The review points out how little we know about the children who are in our care and who are reported as maltreated. Although the literature on the exogenous factors contributing to child maltreatment in out-of-home care is sparse, studying the impact of events outside the walls of the facility, which affects quality of care and the subsequent potential for the maltreatment of children is important. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Nunno, M., Holden, M., & Leidy, B. (1997). Child maltreatment in loco parentis. In J. Garbarino & J. Eckenrode (Eds.), Understanding abusive families: An ecological approach to theory and practice. (pp. 131–141). Jossey-Bass.
Focuses on the maltreatment of children by those adults who are in loco parentis with children in their care. This covers maltreatment within residential facilities that provide 24 hr care to children, such as hospitals, shelters, detention facilities, centers for special needs children, and foster homes. The chapter also examines issues of maltreatment within community-based organizations, such as elementary and high schools, preschools, family day care, and daycare facilities for the entire range of a community’s children. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Holden, M. J., & Powers, J. L. (1993). Therapeutic crisis intervention. Reclaiming Children & Youth: Journal of Emotional & Behavioral Problems, 2(1), 49–52.
Describes a therapeutic crisis intervention program for potentially violent children and adolescents. Staff selection is designed to facilitate management of a child/adolescent in crisis. To attain therapeutic control during difficult crisis points, without sacrificing the dignity of the direct care worker or the patient, the program uses therapeutic crisis intervention principles. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Rindfleisch, N., & Nunno, M. (1992). Progress and issues in the implementation of the 1984 Out-of-Home Care Protection Amendment. Child Abuse & Neglect, 16(5), 693–708. https://doi.org/10.1016/0145-2134(92)90106-2
Assessed the implementation of out-of-home protection programs in the US following the passage of P. L. 98-457 in 1984. 47 jurisdictions were surveyed. All but a few states have changed their statutes or regulations to include a definition of persons responsible for the welfare of the child that is consistent with the law. Compliance by states with federal requirements in this regard means that out-of-home care providers are subject to mandatory reporting of out-of-home abuse and neglect. 29 states reported having information systems in operation, and 19 provided annual reports containing information about out-of-home abuse and neglect. (French & Spanish abstracts) (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Nunno, M., & Rindfleisch, N. (1991). The abuse of children in out of home care. Children & Society, 5(4), 295–305. https://doi.org/10.1111/j.1099-0860.1991.tb00495.x
Discusses methods for identifying, reporting, investigating, and preventing child abuse in out-of-home care (OHC), based on a survey of state representatives to the National Center on Child Abuse and Neglect. Survey results suggest that the investigation of OHC maltreatment should be excluded from the responsibility of child protective services to avoid a conflict of interest when the investigating agency is either the placing or sponsoring agency. To understand the causes of maltreatment in OHC, it is necessary to examine the interaction of the residential environment, the staff, and the children in care. Workshops on anger management, behavior control, and conflict/crisis resolution are essential in training child care workers, empowering both child and child care worker if presented in the context of responding to the children’s developmental needs. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Greene, J. R., & Holden, M. M. (1990). A strategic-systemic family therapy model: Rethinking residential treatment. Residential Treatment for Children & Youth, 7(3), 51–55. https://doi.org/10.1300/J007v07n03_06
Suggests that the strategic-systemic family therapy model provides child and youth care professionals with a residential treatment model that successfully incorporates family therapy with residential child care practice. This model is a set of assumptions about the way problems are conceptualized, the process of change, the client as a part of a social system, and the client–therapist relationship. Assumptions include viewing symptomatic behavior as serving a benevolent, regulatory function in the family, such that attempts to alleviate the symptoms may be resisted on grounds that the system would be left unregulated. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Powers, J. L., Mooney, A., & Nunno, M. (1990). Institutional abuse: A review of the literature. Journal of Child & Youth Care, 4(6), 81–95.
Introduces the social work, child welfare, and child care literature pertinent to the maltreatment in residential facilities. Major theories, research results, and state and federal policies addressing the phenomenon are presented. Issues that are addressed include the scope of the problem, definitions, and the relationship to familial maltreatment. Problems of identifying and reporting institutional maltreatment are discussed, especially as they relate to the accuracy of incidence data. Potential causes of maltreatment are described including the role of victims, perpetrators, organizational structure, and environment. (PsycINFO Database Record (c) 2016 APA, all rights reserved)
Nunno, M. A., & Motz, J. K. (1988). The development of an effective response to the abuse of children in out-of-home care. Child Abuse & Neglect, 12(4), 521–528. https://doi.org/10.1016/0145-2134(88)90069-5
Argues that the placement of children in foster or residential care does not ensure that children will be safe from abuse or neglect. The incidence of out-of-home maltreatment, especially sexual exploitation and abuse, has given rise to new expectations and legislation that has placed the protection of children in alternate care in the hands of the child protective system. Such investigations differ in purpose and scope from familial investigations, and the current protective system is without adequate preparation, policy, and procedures to perform them. The differences in familial and out-of-home care investigations in relation to identification and reporting, assessing risk factors in the initial report, evidence gathering, essential components of the investigation, levels of culpability, and corrective action approaches are discussed. It is suggested that specialized investigation units may be more suited to these investigations than traditional child protective services. (French & Spanish abstracts) (PsycINFO Database Record (c) 2016 APA, all rights reserved)
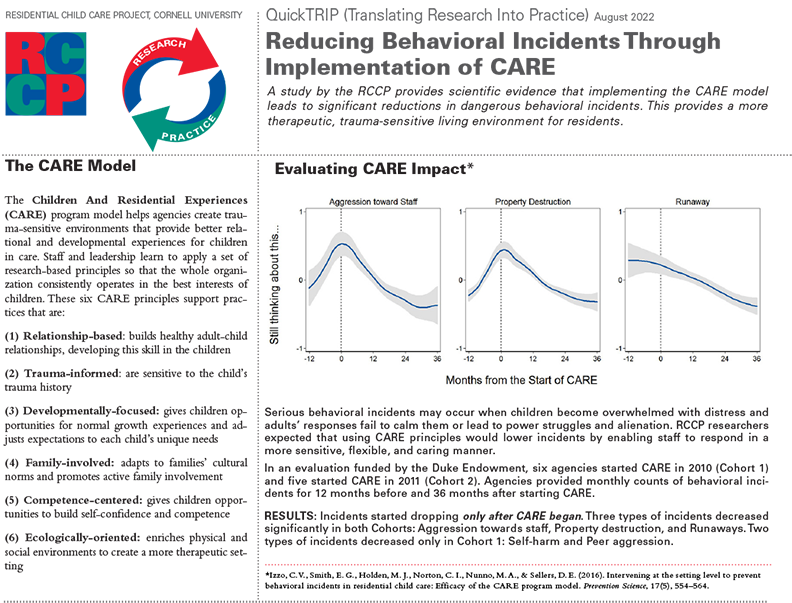
Above is page 1 of the Reducing Behavioral Incidents Through Implementation of CARE QuickTRIP, August 2022. Download the entire QuickTRIP in .pdf format.

Above is page 1 of the Exploration of the Youth-Adult Relationship in Residential Care QuickTRIP, August 2024. Download the entire QuickTRIP in .pdf format.
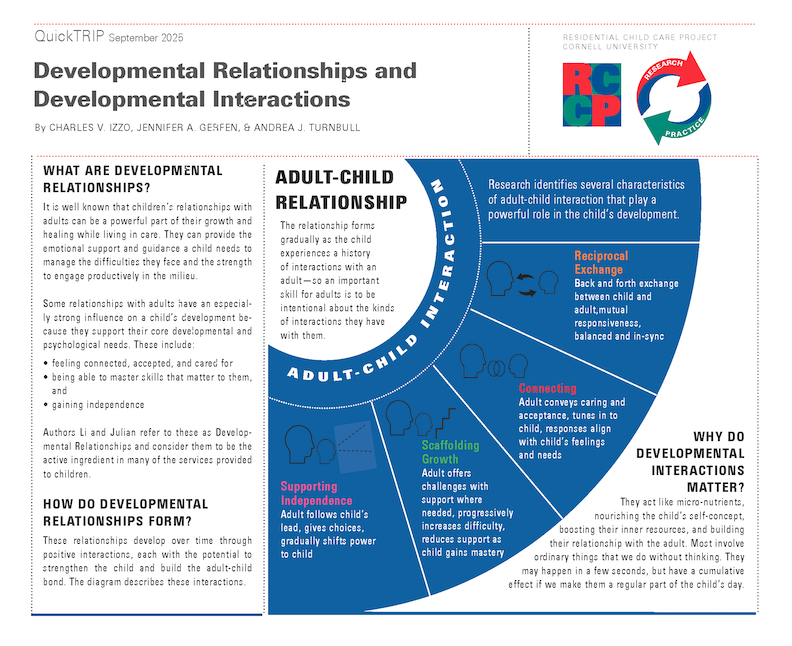
Above is page 1 of the Developmental Relationships and Developmental Interactions, September 2025. Download the entire QuikTrip in .pdf format.





QuickTRIPs: Translating Research into Practice
The RCCP's mission includes applying new information, gained through research, into recommendations that practitioners can use. RCCP researchers have prepared QuickTRIPS, 2-page documents that translate the practical implications of research studies, for this purpose. Click the title below to view and download the QuickTRIP (pdf format):
Developmental Relationships and Developmental Interactions
Exploration of the Youth-Adult Relationship in Residential Care
Reducing Behavioral Incidents Through Implementation of CARE
What Do We Know About Children Who Have Died from Physical Restraint in the United States
Overcoming Challenges with the The Life Space Interview
RCCP Publications
Note: To view the abstract, click on the article title.
2022
2021
2020
2019
2017
2016
2014
2013
2012
2011
2010
2009
2008
2006
2003
1997
1996
1993
1992
1991
1990
1988
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
©2021 Residential Child Care Project, Cornell University, Ithaca, New York USA